
Introduction
Wiring New Connections
- Definition of Neuroplasticity
- The Three Rules of Neuroplasticity
- R.A.F.T.
- Persistent vs Acute Pain
- Brain Access
- Learning Pain
- Hub Treatment
- Active and Passive Treatments
- Provider and Patient Roles
- Counter-stimulating Pain
- Shrink the Map
- M.I.R.R.O.R.
- N.O.R.M.A.L.
Definition of Neuroplasticity
Look at pages 4 and 5 of the Neuroplastic Transformation workbook. They are a nice introduction to the vast amount of information your brain receives from your body and then uses to tell your body what to do. The complexity of the brain may seem overwhelming, and it does its job so well, that people tend to assume that it can accomplish whatever it needs without help. When it goes awry, however, the brain needs to be directed to get back on track. Truly, there are massive changes happening in our brains all of the time. Think about the fact that the adult brain makes and breaks 7.5 trillion synapses a week.
We literally change who we are week after week. It is even more astounding that we are able to maintain a continuity with all these changes, but that is exactly what the brain does. Somehow the brain knows how to remain constant enough to provide a day to day connection to oneself, while changing both itself and the body so much that we appear and act very differently as time goes on.
The Three Rules of Neuroplasticity
Where persistent pain is concerned it is important to remember the three rules of neuroplasticity, because not only is pain something that is learned, but that learning requires those rules. Review them on page 5 of the Neuroplastic Transformation workbook. Although it is hard to believe that we can use such simple approaches to change something so profound and life-altering as persistent pain, it is a fact. Remembering to use the very intrusion of pain into conscious thought, emotional awareness or physical limitation to counter-stimulate the brain is the key to restoring the appropriate role of pain.
It is actually the most important sensation in our body. Pain keeps us alive by telling us when we have exceeded our limits. It is precisely because it is not there all of the time that pain is so helpful and useful. Unfortunately, when pain persists it loses its ability to warn us of danger, and all we are left with is the unpleasantness and the fear and anxiety that accompanies it.
R.A.F.T.
R.A.F.T. is one of the core concepts of Neuroplastic Transformation Treatment. Review Page 9 of the Neuroplastic Transformation workbook. People living with persistent pain experience phases of their disorder, going through matching phases of treatment. Persistent pain marks the transformation of pain from a symptom that warns about danger to a disease that is marked by changes in the entire body. Injury to tissue is not cleared up by normal inflammatory and anti-inflammatory processes. Nervous System signaling is amplified by unrelenting painful input from the sensory nerves in injured parts of the peripheral body. This results in perpetual firing of nerve cells in the spinal cord and the brain and activation of nerve cell receptors that cause rapid and long term firing of nerves. Inflammatory discharges of non nerve cells in the brain, within which these perpetually firing nerve cells are located, results in expansion of the pain map in the brain, at the cost of other important regional functions.
Inflammatory compounds are released by the brain into the injured peripheral tissue and a loop is set up. Look at the writing under the R.A.F.T. graphic on page 9 of the Neuroplastic Transformation workbook. Review the description of the four phases of treatment, Rescue, Adjustment, Functionality and Transformation. Like the picture of the raft full of paddlers, it takes a team to wend through these phases and there are likely to be many treacherous traps along the way to prevent ending persistent pain’s fury. Diligent and relentless work will overcome obstacles.
Persistent vs Acute Pain
Look at the pictures on pages 10 and 11 of the Neuroplastic Transformation workbook Notice that the areas of the brain where pain is experienced are exactly the same, but that the amount of brain “real estate” dedicated to perceiving pain is expanded with persistent pain. Use the graphics to visualize taking back brain real estate in pain perceiving areas for other functions such as decision making, pleasure, planning, problem solving, autobiographical and emotional memories, pleasant scents, soothing, empathy, other sensations, physical activity. See this animation of brain pain signals changing from acute to persistent, then to pain relief.
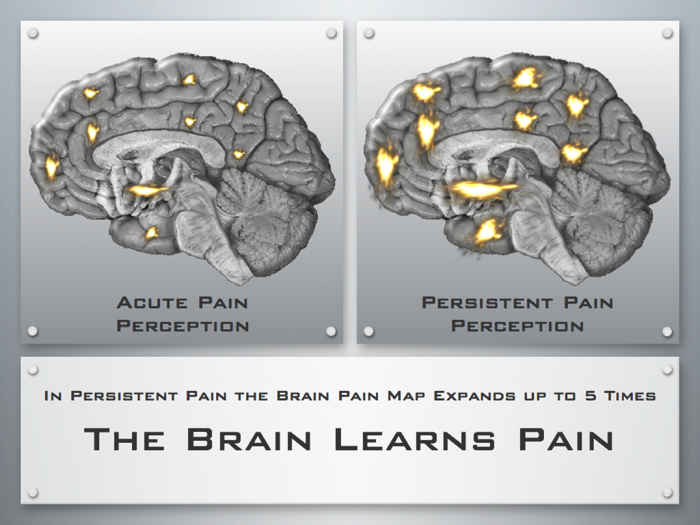
Remember that acute pain goes away. Expect your pain to go away.
Hub Treatment
Neuroplastic transformation is the treatment hub for persistent pain disorders. When pain transitions from a symptom to a disease, it is not merely more pain, longer lasting pain or constant pain. This process is one of neuroplastic adaptation to a stimulus resulting in molecular, cellular, anatomic, physiologic, electrical and functional changes in brain and peripheral body. Varied treatments have been established to deal with the persistence of pain. Some of these are aimed at altering or suppressing peripheral sites and some use more systemic approaches to manage pain. Medication, Invasive, Bodywork and Psychosocial approaches can be used individually or in concert with each other. Multidisciplinary and Interdisciplinary treatment teams may be brought to bear. All of these treatments are aimed at containing and managing the disease of persistent pain. None are crafted to cure the underlying neuroplastic process that has caused pain to transform from symptom to disease. It is only by harnessing the power of neuroplasticity that persistent pain can be resolved.
A wheel without a hub will collapse and fail. By making Neuroplastic Transformation the hub of the treatment for persistent pain, all of the spokes of the wheel become strengthened, unified and focused.

The goal of treatment shifts from reining in pain to reversing the basic forces that have caused it be maintained. Understanding these forces and the stages of treatment harnesses the same power that unleashed pain’s persistence. Instead of these processes occurring randomly based upon runaway input, the incredible access to the brain’s power is used to disconnect expanded pain networks, stop perpetually firing pain-dedicated nerves, resolve the production and release of inflammatory molecules, reverse the energy used to maintain pain receptors and restore normal pain response.
Brain Access
We have more access to the brain than any other organ, even the skin. The brain uses the peripheral body to inform it of everything going on in the external world. It then directs the peripheral body to make adaptations to protect itself, survive and follow the Prime Directive: Avoid Pain; Pursue Pleasure. Every individual uses thoughts, images, sensations, memories, emotions, movement and beliefs to change their own brain. This brain access alters anatomic development, cellular structure, physiologic coordination, electrical circuitry, molecular activity, regional function and neuroplastic change. Everything we do, learn and master results in a change at all of these levels. This incredible access and sweeping change can be effectively used to end the tyranny of pain persistence.
The process of persistent pain is learned. Everything we can do is learned behavior. When we learn something our brains are changing. With each new thing we learn there is a transition from awkwardness to a smooth fluidity of function with lasting and surprising results. While we learn new things our brains are following all of the rules of neuroplasticity: Look at pages 6 and 7 of the Neuroplastic Transformation workbook and the changes that happen in the brain when we learn to read. This is something that we do repetitiously, without really knowing the whole new world that is about to open up for us. In persistent pain the brain uses this repetition to teach us pain. It is telling us that something is wrong, but the solutions it offers are worse than the problem. We have to consciously override the way things are usually done and take control.
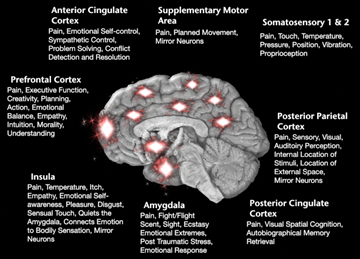
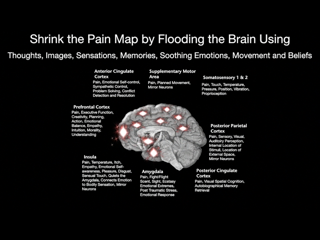
To overcome persistent pain we cannot accept its inevitability. To do so would accommodate an “abnormal” normal. By using conscious access to the brain we can reclaim normal. We can teach our brain to stop pain’s persistence. The graphic on page 13 of the Neuroplastic Transformation workbook shows regional functions in the areas we perceive pain. By stimulating these other functions whenever pain spikes intrude upon consciousness, the pain signaling itself can be used to determine when to use thoughts, images, sensations, memories, soothing emotions, movement and beliefs to access and change the brain. This upends the current model of pain management to one of counter-stimulation, giving persistent pain no quarter, no acceptance.
Active and Passive Treatments
Using this website in conjunction with the Neuroplastic Transformation workbook is a way to expand what is a written guide to something far more. It is also a way to move from being in the role of passive patient to active leader of your own pain treatment team. While passive treatments can be very effective it is critical to shift into a model of active care between treatment sessions by constantly counter-stimulating the brain in response to pain intrusions. Look at page 8 and reread the text. Making the transition to the leader of one’s own care by understanding neuroplastic treatment approaches, completely shifts the pain treatment paradigm and opens a world of possibilities. The ultimate goal moves past pain management to that of life transformation. Go to page 16 and look at the ways real people are applying the use of thoughts, images, sensations, memories, soothing emotions, movement and beliefs to make changes in brain real estate, reassigning nerve cells to other functions by counter stimulating their pain episodes.
Provider and Patient Roles
The current model of pain care tends to place providers in the active role, performing procedures, giving medications, doing body work, intervening psychologically and recommending ways to cope and manage between treatment sessions. Patients are placed in the role of passive participants during treatment sessions and then often left to their own devices to play a more active role between sessions. Neuroplastic Transformation treatment approaches change this model of care. It remains important for providers to come up with a treatment plan and to use the professional training and skills they have to help people with persistent pain. The change here is that providers also help the patient to move toward the position of leadership in this relationship. To accomplish this the care provider must give patients specific things to try between sessions and follow up on these things when the patient returns for care. From the patient’s perspective, this would mean that the patient needs to take the provider’s ideas and dig into these to see what really works for them. Staying with old approaches, even helpful ones, because of a fear of trying something new must be put aside, as the brain focuses upon novelty. Going beyond ones interests and limits can open up entire vistas of new approaches. Providers have to allow and encourage patients to bring their ideas back to treatment to hone and refine these.
This website has animations and videos keyed to specific sections of the workbook, such as this video. There are also separate animation and video (Pain Bytes) Sections of this website that may be useful. At the end of each section of the workbook we have a page called Neuroplastic Tips. Here we make very specific suggestions related to the section. We recommend that you try these and go beyond your current comfort zone, by trying things within your physical abilities to challenge and delight your brain. We have also worked to provide products that are helpful to make neuroplastic change. These products have been carefully thought out and tested to be useful for many people who live with persistent pain. These are located on the Products section of the Neuroplastix site and we have incorporated neuroplastic education into each of these.
Counter-stimulating Pain
The graphics on page 10, 11, 12 and 13 are some of the most important ones in the Neuroplastic Transformation workbook. On page 10 we see the 2 regions in the spinal cord and 16 regions of the brain that make up the pain circuit. This depicts acute pain where 5% of the cells in each region are dedicated to pain processing. These nerve cells are reserved for pain and are shut off, until signaled by sensory pathways in the body to turn on due to danger in the form of injury, illness or inflammation. These signals are processed from the back part of the spinal cord, crossing over to the opposite side of the cord and sent up pathways to the brain stem and mid-brain. We only perceive the signal as pain after it reaches the thinking brain. Here in the 9 regions of thinking brain where the signal is received we experience it as pain. In acute pain some of the same regions and a few different ones send a signal back down to the spinal cord to intercept the incoming signal and shut off the pain so that it never reaches that upper part of the brain, which we use to perceive sensations. On page 11 we see the graphic that shows the same regions in the spinal cord and the brain being simulated, but this time the signal covers a greater area. This represents the recruitment of other nerve cells to expand the pain map and steal away cells from other regional processes. This is a basic principle of neuroplasticity. The brain assigns cells to specific functions, but if one function becomes more active, cells are taken from other functions to strengthen the more active one
Look at these two pictures on page 10 and 11, turning the pages back and forth. The picture on page 11 shows one of the key reasons why persistent pain is no longer a symptom, but has transformed to a disease. This is not because the pain is chronic, but is that expansion of brain real-estate to 15% to 25% of the cells in these regions that are processing the pain signals. Now look at the graphic on page 12. Here we see that even in wound-up and persistent signaling below the upper 9 regions of the thinking brain, if the signal does not advance into the thinking brain, there can be no pain. Turn page 11 and 12 back and forth and recognize that if the signal stops below the upper 9 regions of the brain, there can be no pain. Keep looking at the graphics on page 11 and 12 until you can memorize the difference and visualize them without the actual pictures. Remind yourself that if your brain looks like the graphic on page 12 you cannot have pain.
Shrink the Map
The key graphic of the entire Neuroplastic Transformation workbook is that on page 13. This shows all of the perceptive areas of the brain where persistent pain expands the pain map, as well as many of the other functions in these same area that are being over-run by pain perception and pain stimulation. At the top of the page are the instructions to Shrink the Map, by accessing the brain with thoughts images sensations memories, soothing emotions, movement and beliefs. It is important to understand that these ways we access our brains are the keys to stopping persistent pain. The more consistent and robust the counter-stimulation to the pain the more we can take back real estate for these other functions. From simple thoughts to different sensory inputs we can teach our brains to move the relentless, persistent and constant pain signaling to comfort and pleasure.
The key is to not let any pain signaling go by without opposing it with other signals. Remembering that we learn everything by repetition and consistency reinforces the notion of always counter-stimulating the pain. Reviewing the patient experiences of opposing pain, helps with the ideas others have successfully used and gives the reader the opportunity to come up with their own way of achieving pain control.
M.I.R.R.O.R.
We have come up with an approach to treating persistent pain that is based upon the principles of neuroplasticity:
- Continued firing of a nerve by another nerve increases the strength of the firing and the number of synapses dedicated to those nerves. (What gets fired, gets wired)
- Nerve cells that do not fire other nerves over time will lose synaptic strength and break synapses dedicated to those nerves. (What you don’t use, you lose)
- To conserve the amount of energy the brain uses, old synapses must be broken, when new synapses are formed. (When you make ‘em you break ‘em; when you break ‘em you make ‘em)
The brain changes constantly from conscious input and purposeful activity to information processing that happens automatically and without any self-directed stimulation. As stated earlier massive changes in synaptic connections occur throughout life and any new activity or learning changes the brain’s anatomy, physiology, cell structure, synaptic strength, electrical circuits and regional functionality. This may also leave a vulnerability to runaway processes, resulting in neuroplasticity creating a disease state. At the same time an opportunity is created to actively use neuroplasticity for something that works as an agent of positive change. Even a process that happens below the level of the conscious, thinking and perceiving brain, can be influenced by a desire to change it. In fact all new learning is based upon modifying what is already in place, then through repetition and mastery making most of that learning unconscious and automatic. Through repeated awkwardness and failure a person is gradually rewarded with a fluid ability to perform the necessary tasks, that consistently work. In fact, when something is mastered, it is surprising when it does not work. The more it is repeated and becomes part of the regular living routine, the less conscious attention it requires to perform and the higher the level of performance.
The idea called MIRROR applies these concepts. This stand for:
Motivation
Intention
Relentlessness
Reliability
Opportunity
Restoration
Review the text on Page 14 of the Neuroplastic Transformation workbook. Utilizing these basic principles to rebalance pain processing circuits, the brain can restore normal pain perception and control to people suffering with persistent pain. This requires a few shifts in beliefs that are held about pain. Pain is not something that controls us. Pain is not the inevitable fate of those with persistent pain. Persistent pain is not the result of damage to the body tissue. Pain is not experienced in the body, but is experienced in the perceptive part of the brain. The body does not act independently from the brain, and the brain relies upon the input from the body to make all of it’s own changes. Normal activity does not damage the body after an injury has healed. Regardless of the source of the injury, we have many opportunities to consciously change our pain perception. Learning to control persistent pain is no different than learning anything else. Persistence, practice and failure will ultimately lead to mastery and control, if one remains relentless in one’s pursuit of pain control. Pain management is not the goal of treating persistent pain. We can work toward a reasonable expectation of curing the disease of persistent pain. While a person may not be able to cure the underlying disease or injury in persistent pain problems, with this approach, one can learn to shift the pain from the pain persistence to the symptom of acute pain, that is pain that occurs because we have exceeded a limit and when that excess is corrected, returns to a baseline of painless living.
N.O.R.M.A.L.: Neuroplastic Optimization and Reduction of Medication for Adaptive Living
The polypharmacy of pain treatment is criticized for side effects, drug-drug interactions, worsening pain states, dependency, addiction and even inadvertent death. The problem is not with the medications, but in the way they are utilized to treat persistent pain. They have become the core treatment for this disease process. If the dynamics of persistent pain are recognized as a neuroplastic process, we must view neuroplasticity as the basis for persistent pain and it’s treatment. All treatment should be aimed at creating neuroplastic change to oppose and halt the process of persistent pain. Medications are an excellent way to alleviate symptoms while working on the underlying cause, but cannot be the mainstay or central principle of any treatment program. They are a spoke in the wheel of treatment options with neuroplastic treatment at the center.
People living with persistent pain often end up on a long list of medications designed to treat a host of pain-related symptoms and medication-induced side effects. Over time, this becomes the primary treatment people receive. While medications can be effective alone and in combination, they have many drawbacks. Medication management often promotes a passive patient model of care and undermines people taking an active role in their own recovery. The body and brain adjust to the medications, and they become less effective. Visits to pain practitioners then consist of changing or rearranging medication regimens. Patients may improve for a time, but a vicious cycle of short-term improvement with subsequent worsening of symptoms occurs due to tolerance, requiring more medication. Side effects and drug-drug interactions further complicate the situation, and the body’s own ability to stabilize, rebalance and return to normal is impaired. It reaches a point where it is unclear whether a patient’s problems are due to their underlying pain disorder or the effects of long-term medication use.
By design, medications mask symptoms. It is these very symptoms that provide the clues to possible treatment solutions. By relying on medications every time pain increases, the opportunity to evaluate other pain relieving treatment options is lost. Anxiety and a fear of pain ensue rather than a sense of curiosity about what is happening and what might help. People maintained on chronic medications tend to do less, contract their lives, sense and report higher pain, depression and anxiety levels. Mutual patient and practitioner goals should be the prudent reduction of medications within a more active, patient-centered program based on neuroplasticity.

Medications can then take their rightful place and be used most effectively. They play a prominent role in the Rescue and Adaptation phases of treatment and take on a secondary role when the patient advances to the Restoration and Transformation phases. In the Restoration and Transformation phases patients are actively applying neuroplasticity techniques to change their pain and medications can be used as needed for relief of symptom exacerbation
As part of the Neuroplastic Transformation treatment program, the gradual and thoughtful reduction of medications is employed. It is called Neuroplastic Optimization and Reduction of Medication for Adaptive Living or N.O.R.M.A.L. When people take control of the neuroplastic processes that created the pain disorder, pain decreases and a great sense of self-control replaces the feeling of being the victim of persistent pain. At this point, medications can be reduced gradually and continued neuroplastic approaches can hone and improve self-directed pain and mood control guiding the process of transformational living through pleasurable experience.