
Neuroplastic Brain and Body
Wiring New Connections
- No Brain, No Pain
- Wind-up Pain
- Learning Persistent Pain
- Resetting the Alarm
- Astrocytes and Fibroblasts: Hidden in Plain Sight
- Brain-Body Loop
- Hit the Brakes on the Pain Train
- The Brain’s Connective Tissue System
- Who is In Charge?
- Defending the Fortress
- The Adaptive Barrier
No Brain, No Pain
Pain is processed and perceived in the brain and felt in the body. Signals are sent from the body, the brain processes them, locates the signal input and responds in various ways. The person perceives the sensation and the body reacts via the brain’s directive. Almost every stimulus perceived by the brain is transmitted via the spinal cord. It may be painful or non-painful stimulus based on the intensity of the signal and the type of receptor in the body that is activated. Pain is a warning of danger threatening a person’s survival in a normal setting. The perception of pain is not a bad thing. The sensation of pain feels bad but it is essential to survival.
Traditionally, the transmission of pain is presented as occurring only through the electrical signaling from the body through the spinal cord to the brain and back out again. In reality, pain signal transmission occurs instantaneously and simultaneously at multiple levels via various chemical and cellular reactions. Still, the brain processes and perceives and the body senses. Said another way, what we feel in the body is what we perceive in the brain. The two are one thing.
Wind-up Pain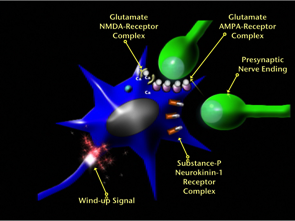
Wind-up pain is one of the hallmarks of the neuroplastic changes that create persistent pain. Persistent pain is not just a longer lasting acute pain. There are several changes that happen in brain and body. Wind-up can happen anywhere in the spinal cord or brain. It means that the pain signal that comes into the central nervous system becomes stronger and longer lasting. This is a physiologic process that involves activation of receptors that are normally dormant on post synaptic nerve endings. The result is that the nerve fires more frequently and with greater strength. It also means that the nerves fired this way keep firing even without an ongoing stimulus. Hence people may heal, but the pain circuit remains activated.
Part of the wind-up process involves nerves sprouting into pain processing areas that normally transmit signals that do not lead to pain. The result is that nerve signaling for touch, movement, pressure, temperature or vibration signal for pain. These sprouts also grow into different levels up and down the spinal cord. This accounts for pain starting in a discreet area and progressing to occurring in an entire region. In this way an injury to the finger causing local pain can gradually involve the entire hand.
Look at the graphic on page 26 of the Neuroplastic Transformation workbook and read the accompanying text. The graphic shows an incoming signal that winds up at the dorsal horn of the spinal cord. This signal is not yet felt as pain, because it has not reached the thinking and perceiving part of the brain. When it does so, it will wind up at each of these levels due to activation of NMDA receptors on post-synaptic nerve endings. This is one of the reasons that persistent pain is so powerful.
In persistent pain there are many signals sent to the brain, including touch, temperature, movement, position and vibration that are all being interpreted by the brain as pain. See if you can distinguish these normally non-painful signals and separate them from your pain. Instead of viewing your pain as a danger to avoid, look at it as something that is no longer dangerous and instead as a signal to do something, in order to come up with new ways to reduce it. By doing this the pain can be reduced from a threat to an opportunity to change your brain in relationship to your body.
Learning Persistent Pain
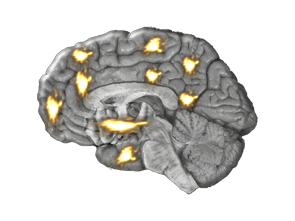
Look at the graphic on page 27 of the Neuroplastic Transformation workbook. It shows one of the main differences of acute and persistent pain. The same 9 regions of the brain involved with pain perception are activated in acute and persistent pain, more real estate in these regions is dedicated to pain, however, when it becomes persistent. This expansion of the pain map sets up pathways involving molecules, brain cells, circuits and networks that make the person involved more susceptible to developing persistent pain later in life with other physical and emotional trauma.
While brain networks physically wire new synapses to connect to each other, they also connect via rhythmic frequencies. This means that large networks in the brain influence each other through both direct physical connections of synapses, as well as mutual rhythmic linking of electrical activity. Lower frequency linking exemplifies network coherence and coordination. Higher frequency resonance between networks means disruption. The Default Mode Network (DMN) has both an anterior part in the front of the brain and a posterior part in the back of the brain. When pain stimuli ramp up frequencies between the Fronto Insular Network (FIN) and the anterior DMN a disruption of one’s sense of self occurs.
Resetting the Alarm
Pain is meant to be an alarm system that warns a person of danger that will cause harm or destroy the body. It is the way we survive our environment. That all changes when pain becomes the disease process that creates alterations in nervous system structures, transmission of signals and pain perception and sensation. Persistent pain signaling and processing becomes the main event taking place in the body. It recruits neurons in the brain and allocates increased energy to maintain itself. The only way to overcome this process is to reverse it by repetitively and relentlessly activating the brain with counter stimulating and soothing signals. In this way, pain can take its rightful place and become a danger signal once again, rather than being the danger itself.
Astrocytes and Fibroblasts: Hidden in Plain Sight
Astrocytes and fibroblasts are rarely considered in health or disease despite the fact that they are the most numerous cells in the brain and body, respectively. Astrocytes coordinate the workings of the neurons and dictate nervous system responses. They do so chemically rather than electrically. Fibroblasts monitor the status of processes in the body and either act as maintenance cells or mount an inflammatory response in the face of injury or infection. They both function elegantly to protect, maintain and defend balance and health.
Brain-Body Loop
The brain-body loop describes the constant connection between body and brain. Where pain is concerned it involves both the suppression of acute pain and amplification of persistent pain. It is a two way communication between the Connective Tissue System and the Nervous System.
In acute pain, the nerve cells pain processing regions of the brain fire due to input from peripheral tissue. Some of these nerve cells send signals to the spinal cord to suppress the incoming signal. There is no pain when the injured tissue is at rest. Pain is re-experienced if a person stresses the injured tissue. Higher functioning regions of the brain send signals to stop the pain and return the tissue to healing. Inflammation in the peripheral tissue gradually stops and is replaced by an anti-inflammatory response. Growth factors are released to repair the extracellular matrix and local nerve endings. Once this occurs, pain signals to the brain desist. Use of that tissue returns to normal and painless function.
The brain-body loop works quite differently when pain becomes persistent. Signals coming in from the peripheral nervous system increase in the central nervous system. This is known as wind-up. A series of events occur leading to runaway firing of nerves with or without input from the part of the body that is injured. The brain tries to suppress the signal, but it is too powerful. Brain astrocytes release inflammatory molecules. Nerve cells release more of the main pain neurotransmitter, Substance-P. Higher levels of Substance-P expand the network of pain transmitting nerves. Higher functioning areas of the brain signal to stop using that part of the body, regardless of its state of repair. Inactivity and disuse lead to loss of function and local release of more inflammatory chemicals. Substance-P is sent out to the peripheral tissues, functioning as an inflammatory substance. Local anti-inflammatory responses are overwhelmed. This results in ongoing inflammation, increased pain signals to the brain and augmentation of the brain-body loop.
Hit the Brakes on the Pain Train
Nerve cells behave in various ways to serve the purpose of normal functioning of the brain and body. These are Short Term Potentiation, Short Term Depression, Long Term Potentiation and Long Term Depression. Look at the graphic on page 29 of the Neuroplastic Transformation Workbook illustrating these processes.
One of the major ways pain becomes a disease is when nerve cells continuously fire with or without input from any other nerve cell. This is called Long Term Potentiation. These nerves are essentially runaway cells firing on their own and wiring other cells into their network to do the same thing. Left untreated, pain networks grow and pain increases. Traditional modalities to block or suppress this process are helpful in the beginning phases of treatment but long term solutions must be aimed at stopping and reversing the process. Incorporating neuroplasticity techniques as the hub of treatment provides a way to move beyond suppression to resolution.
Studies have shown that Long Term Potentiation can be converted to Long Term Depression by another nerve firing slowly in proximity to the rapidly firing potentiated nerve. Long Term Depression aborts the persistent pain process. Neuroplasticity techniques using this approach to reset the circuits should be able to convert Long Term Potentiation to Long Term Depression in much the same way.
The Brain’s Connective Tissue System
Astrocytes, microglia and oligodendrocytes are cells collectively known as glia. Ninety percent of all brain cells are glia. Structurally, they create the matrix that suspends the nerve cells in the brain. Their purpose does not stop there. The glia coordinate function, facilitate communication between brain and body and monitor and modify input and output. The graphic on page 30 of the Neuroplastic Transformation workbook depicts the various brain cells. All glia have counterpart cells in the body that interact similarly to the way the glia interact in the brain. The glial cells are part of the connective tissue system that exists throughout the entire body. The nervous system is classically viewed as the way the brain and body are connected. In reality the Nervous System and the Connective Tissue System are one system that elegantly orchestrates communication allowing for instantaneous processing of input and output.
Who is in Charge?
There two types of cells in the brain. They are nerve cells and glia. The interplay between these two cell types allow for the seamless processing of information. Increasing understanding of how glial cells function demonstrates their critical role in monitoring, modifying and managing the intricate processes that take place in the nervous system, immune system and circulatory system.
There are three types of glial cells. They are astrocytes, oligodendrocytes and microglia. Nerve cells in the brain are all imbedded in astrocytes. This allows them to pass molecules and electromagnetic waves to one another and modify brain activity. Look at the graphic on page 30 of the Neuroplastic Transformation workbook and review the text. The graphic shows the relationship of the various brain cells and the text describes in detail the numerous functions of astrocytes. From altering the amount and spread of neurotransmitters to coordinating placement of newborn neurons, astrocytes play a critical role in brain function. The oligodendrocytes in the graphic are the cells that wrap around the long shafts of nerve cells, called axons. They make a fatty substance known as myelin that coat the axons. The more myelin, the faster the electrical signal. Microglia are responsible for protection of the brain from foreign invaders, injuries and toxins. They also trim old synapses being replaced by new synapses.
Defending the Fortress
Molecules in the bloodstream pass through the circulatory system directly into the brain via the Blood Brain Barrier (BBB). The BBB is a highly selective network of specialized capillaries, astrocytes and microglia. It functions to keep out destructive substances and mounts the first response aimed at destroying invaders. There are three layers of the BBB. Layer one is composed of capillaries and lets only the smallest substances pass in and out of the brain. Astrocytes comprise layer two. Astrocytic projections or “feet” wrap around the capillaries and strengthen the barrier. They respond to unknown substances with a massive release of inflammatory cytokines that attack the substances and call forth other microglia. The microglia are the third layer of the BBB. They attack anything suspicious with a pinpoint barrage of inflammatory chemicals aimed at destroying the substances.
Look at the graphic on page 31 of the Neuroplastic Transformation workbook. It shows a capillary in the brain running through an astrocyte. Every nerve cell, capillary, microglial cell and oligodendrocyte are contained within astrocytes. Look at the graphic on page 30 of the workbook.
The Adaptive Barrier
One of the most startling aspects of the Blood Brain Barrier is that part of it actually serves as a gauge to read what passes through the brain’s circulatory system, but never enters into the brain tissue itself. By being able to read these molecules zipping by in the bloodstream, the brain can match these in areas that are deficient in the brain and make pinpoint releases where these molecules are lacking. Thus the brain changes itself in specific areas and directs the body to change itself in specific areas as a consequence of these changes. If we lacked this function every change in the brain and body at a molecular level would be global, resulting in chaos and a breakdown of order so profound that none of us could survive. Read the last column of text on page 31 of the Neuroplastic Transformation workbook for a more detailed explanation of this phenomenon.
Brain Flush
When we sleep the Blood Brain Barrier becomes something entirely different. Beneath the tissue that covers the brain (the Meninges), Every part of the brain is buried in Astrocytes. Astrocytic feet wrap around all structures. The graphic on page 31 of the workbook shows a capillary surrounded by these astrocytic feet. For the sake of illustration, the capillary appears to emerge from this forest of astrocytes. The truth is that the huge network of capillaries in the brain is completely surrounded by astrocytes. The capillaries bring nutrients and oxygen to the brain and remove waste products and carbon dioxide from it. The question arises as to how this waste is removed, in light of two facts. First, the brain, a three pound organ, burns 20% of the body’s energy, leaving behind a massive amount of waste material to be eliminated from the brain. Second, the capillaries in the brain have no loose junctions between cells, making it impossible for the brain’s waste material to be transferred to the general circulatory system by the normal passive diffusion process that occurs throughout the rest of the body.
It turns out that when we sleep the Astrocytic feet pull back from the capillaries by 30% and create channels between the astrocytes and the capillaries. The Cerebrospinal fluid from deep in the brain’s spaces (ventricles) and beneath the brain’s meninges, rushes into these channels at 16 times normal speed, flushing waste from the brain’s tissue. This high speed motion of cerebrospinal fluid creates a downward pressure on the capillaries and forces the waste material through the tight junctions of the capillaries, dumping it into the general circulation. There it is removed by kidneys and liver and eliminated from the body. Literally, the brain flushes itself clean while we sleep.